A post from Ace copied and pasted here:
"Sierra, I am a 52 year old man that was diagnosed with obstructive apnea. I also have astma, but not central apnea.
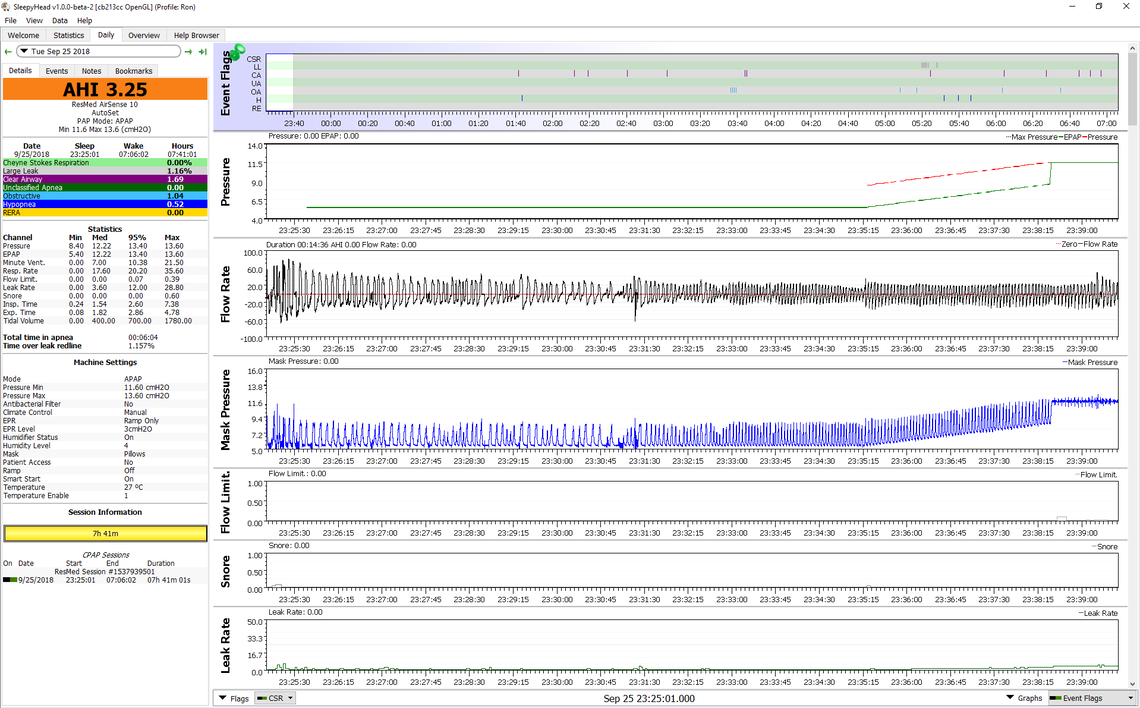
I use the RESMED airsense 10 since one year approximately.
The healthcare detected high blood pressure cause of apnea. And since I got the apap treatment the blood pressure has gone down. But now when I went through a 24 hour test I've noticed that the blood pressure is high during awakening.
I've also noticed that I can wake up a couple of times catching my breath........ when I'm half awake, so to speak, it's almost like I have central apnea.
This is quite scary, when you find yourself not even atempting to breathe.
What sleeptech is writing is not to be taken lightly. The industry itself will never bring up matters like this. Obviously they want to develop their products to be as good as possible to be competitive and sell more. But during development there will be issues like this. And these "issues" can actually cost lives(!)
Now to my point. I've tried with decreasing the EPR-level from the preset level 3 to 2, 1 and finally the last weeks turning it off.
When the EPR turned off completely, I've noticed a very big difference. I breathe much better and sleeps better. My natural brething (respiratory effort) is normal again.
If the EPR-funtion (Expiratory Pressure Relief) affects and increases the CO² levels creating central apnea we should never even consider trying out the EPR(!)
As sleeptech mentioned: "should be avoided in almost every instance."
Concering CO²-levels and central apnea: "I have recorded evidence of this happening."
"Where I work, we only ever allow our patients to use EPR or C-Flex if they have had a sleep study with it and we can verify that it is not causing any harm. Otherwise we do not use it at all. I can think of fewer than 5 people who have actually had some benefit from using EPR/C-Flex in all my years of being a sleep tech."
Please take his warnings seriously.
(For comfort, setting the ramp with EPR is of no harm obviously.)"
My reply to your post:
Based on my personal experience when I awaken during the night short of air, I believe I have had an apnea. It could be either central or obstructive. I unfortunately suffer from more central apnea events than obstructive, and increased pressure is of no benefit in reducing central events.
I have also adjusted EPR from none to 3 on numerous occasions. As I said in my post, it has had no repeatable impact on my frequency of central apnea. But also as I said I can get the same apnea normalization with less maximum mask pressure when EPR is turned off. On that part I agree with Sleeptech. It has some negative impacts but I would suggest it is in mask pressure not any impact on central apnea frequency.
With respect to impact on oxygen and CO2 levels I think you have to put it in perspective. We are talking about a pressure increase of 3 cm of water. Yes, that means more oxygen will go into the lungs, but the question is whether or not 3 cm is significant. I won't bore you with the math, but if you do it the atmospheric air pressure when the weather changes from a low pressure formation to a high pressure formation, the pressure in CPAP units changes by about 35 cm of water. That is a factor more than 10 times higher than turning EPR on or off at a setting of 3 cm. My conclusion is that 3 cm is not significant in the scheme of things. Also remember that standard atmospheric pressure is about 1030 cm of water in absolute units. A change of 3 divided by 1030 results in a very small percentage change.
You mentioned that you gained some benefit by turning EPR off. Again without going through my previous post again, I think that is quite possible in that depending on how your machine is set up turning EPR off may reduce the frequency of obstructive apnea. Have you quantified what your before and after central and obstructive apnea frequency was? I find one needs to document at least a month's worth of data to determine what the change had been.
Another thing to consider is that one of the treatments for higher than 5 AHI due to central apnea is to use a BiPAP machine. A BiPAP really only differs from an APAP in that it can use an EPR of higher than 3 cm. Yes it is called pressure support but it is really the same thing -- a split in the IPAP and EPAP pressures. And central apnea is actually treated by using a higher than 3 cm split in the pressures. Some question the effectiveness of it, but it is done. I know because I suffer from central apnea and I have investigated all options to deal with it including a BiPAP and an ASV machine.
So I will say again that I agree with Sleeptech in that there are some downsides to using EPR for someone who is mainly suffering from obstructive apnea, but causing central apnea is not a very likely one. It certainly has not been my personal observation although I wish it was. I don't think you will find credible sources elsewhere that suggest it causes central apnea either. If there are, I have missed them. If you have them, then I certainly would be interested in looking at them.